Outdated or Unsupported Browser Detected
DWD's website uses the latest technology. This makes our site faster and easier to use across all devices. Unfortunatley, your browser is out of date and is not supported. An update is not required, but it is strongly recommended to improve your browsing experience. To update Internet Explorer to Microsoft Edge visit their website.
Effective May 2026
This policy describes the hearing aid process, key considerations for DVR case facilitators, payment rate determination, and related services such as maintenance and repairs.
When purchasing hearing aids, careful evaluation is essential. The DVR case facilitator must review all ongoing costs and long-term responsibilities with the consumer, including potential cost increases, follow-up appointments, routine maintenance, batteries, repairs, and future replacement needs.
Note: For cochlear implants please follows the Provision of Medical Restoration Services Traditional & Non-Traditional policy.
DVR staff are encouraged to consult with Advanced VRCs, VR Supervisors and Directors, local WDA SenseAbility representatives, and the SenseAbility team (DVRSenseAbility@dwd.wisconsin.gov) for guidance as needed.
If at any point in the vocational rehabilitation process a consumer shows signs of or mentions hearing loss, the DVR case facilitator should ask questions to assess the consumer’s functional hearing in relation to their current work environment, IPE goal, and participating in DVR services.
During Referral and Application status:
During IPE Development/Initiation of IPE Services:
Confirm that hearing aid/s and related services are necessary and appropriate to achieve the IPE goal.
If it is determined that hearing aid/s (new or replacement) and/or related services may be necessary to achieve the IPE goal, proceed with the next steps.
The hearing evaluation process includes several steps; consumers with a history of hearing loss and prior hearing aid/s use may require less information.
Comparable benefits (e.g., Medical Assistance, private insurance) must be identified before purchasing services, including hearing aid evaluations, when doing so will not cause significant delays (e.g., job loss).
Hearing evaluations may or may not be covered by insurance; if the consumer has insurance, they should determine coverage for hearing evaluation with audiogram (if updated one is needed) and hearing aid recommendations.
If the consumer has not had a recent evaluation, refer to a licensed audiologist for a hearing evaluation and/or hearing aid evaluation (these may be done separately).
DVR must use a licensed audiologist—not a certified hearing aid dispenser or unlicensed vendor—to evaluate a consumer’s hearing needs. Refer to Fed Reg 801.109 for more information.
The hearing aid evaluation should include:
Evaluation results and recommendations:
Selection and fitting:
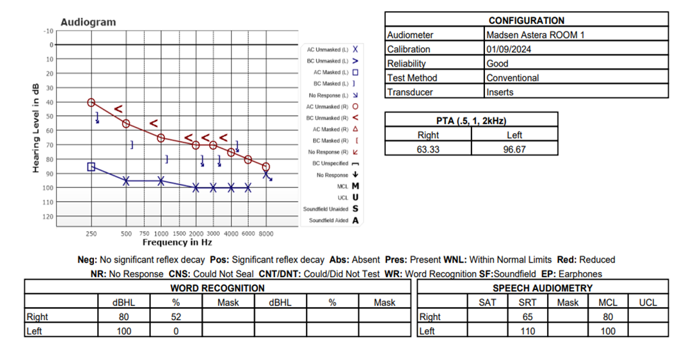
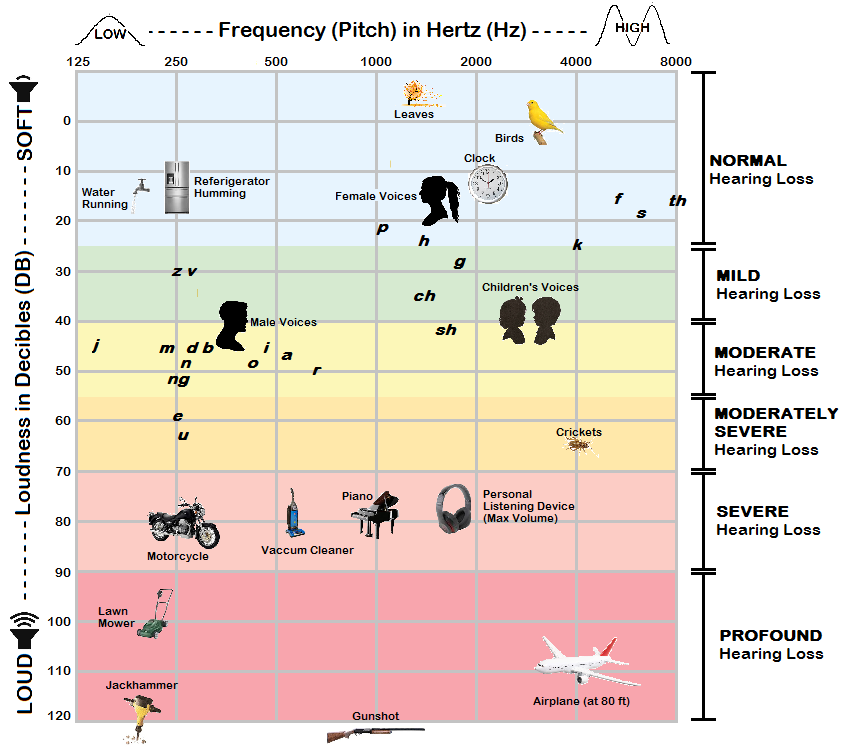
Note: Refer to section 7. Resources and Definitions for information on how to read an audiogram including an example of a standard and functional audiogram.
If hearing aid/s are recommended, proceed with next steps.
DVR’s maximum contribution is the least-cost option or lowest competitive quote obtained. Comparable Benefits (e.g. insurance) may or may not be less costly than MA Maximum Allowable Fee Schedule rate or invoice + 15% (plus Medicaid rate for dispensing fee). If an exception to this policy is needed or there is a concern about a delay in service, consult with your supervisor.
Hearing aids may not be covered by insurance; if the consumer has insurance, they should determine coverage for hearing evaluation, audiogram, and hearing aids/devices.
The scenarios below provide examples of how to apply comparable benefits (insurance coverage) when determining the least-cost option in hearing aid funding decisions.
Scenario 1:
Scenario 2:
Other potential comparable benefits include:
Once pricing has been determined, quotes are attached to the case (as appropriate), and the hearing aid/s and related services have been added to the IPE, proceed with next steps.
| Title | Examples and Included Items | Code | Object/Sub-Object Codes |
|---|---|---|---|
| Hearing Evaluations | Hearing Assessments, Audiology Exams etc. | 021 | Service: 8910000 (5712) |
| Hearing Aids | Restoration Hearing Aids, Hearing Aid Related Equipment | 036 | Supply: 8800000 (5700-72) |
| Hearing Aid Dispensing Fee | Includes:
|
036 | Service: 8910000 (5712) |
| Hearing Devices | Rehabilitation Technology Devices (FM Systems, Bluetooth, loop systems, etc.) Note: If the rehabilitation technology is built directly into the hearing aid, code as 036. |
033 | Supply: 8800000 (5700-72) |
To determine WI Medical Assistance Maximum Allowable Rates for hearing aids and related services, use the following resources:
The following are the Medical Assistance maximum allowable rates for hearing aid dispensing fees, as of February 2026:
Receiving and Case Documentation
Daily care and maintenance
Storage and protection
Batteries and upkeep
Replacement
Warranty and lifespan
Following the purchase of hearings aids with DVR's assistance, consumers should identify strategies for funding future hearing aids, including resources to assist with personal savings planning.
Note: DVR staff are encouraged to consult with Advanced VRCs, VR Supervisors and Directors, local WDA SenseAbility representatives, or the SenseAbility team (DVRSenseAbility@dwd.wisconsin.gov) for guidance.
National Institute on Deafness and other Communication Orders (NIH)
Hearing Aid Process Flow
American Speech-Language-Hearing Association (ASHA):
The professional organization which grants certification for Audiologists and provides resources around hearing and hearing loss
Amplifier:
The component of the hearing aid that boosts the volume of sound.
Audiogram:
The chart that provides a visual representation of your hearing exam results. The vertical axis measures decibels (volume) and the horizontal axis measures frequencies (pitch). An audiologist documents the lowest decibel level you can hear at each frequency. The line on an audiogram identifies the level of hearing loss for each ear. There may also be a field for speech recognition threshold (SRT) which gives a percentage for the amount of speech the person is able to decipher.
Behind the Ear (BTE) Hearing Aids:
Hearing aid with the majority of its parts contained in a case placed behind the ear and attached to an earmold by a clear plastic tube. Mini-BTE hearing aids are also available.
Bilateral Hearing Loss:
Hearing loss in both ears, which could be symmetrical (the same degree of loss in both ears) or asymmetrical (different levels of loss in each ear).
Bluetooth Technology:
Enables the hearing aid to communicate wirelessly with several devices, including mobile phones, computers, MP3 players, and other compatible products.
Cerumen:
Medical term for ear wax.
Conductive Hearing Loss:
Hearing loss occurring in the outer or middle ear that limits the ability of sound to reach the inner ear. This type of loss benefits the most from amplification.
Decibel (dB):
The unit of measure for sound level or intensity. Normal conversation registers at approximately 60 decibels, and long-term exposure to any sound more than 80 decibels could cause irreversible hearing loss. Since the scale is logarithmic, an increase of 6-10 decibels doubles the volume of the sound. See diagram on page 10 for an example.
Degree of Hearing Loss:
Hearing loss is generally classified as:
Digital Signal Processor:
A special microprocessor inside of a hearing aid that manipulates and enhances sound.
Directional Microphones:
Microphones that can focus in on sound coming from a specific location while minimizing background noise.
Earmold:
A piece of plastic, acrylic, or other pliable material that is shaped to the contours of an individual’s ear, used for the fitting of hearing aids.
Frequency:
Represents pitch as measured in hertz. Picture moving up the keys on a piano, from left to right (low-frequency/pitch to high-frequency/pitch). See diagram on page 10 for an example.
FM/DM System:
A device (not a hearing aid) used to amplify sounds and transmit audio from a speaker (transmitter with microphone) to a listener (receiver with earbuds, headphones, or neckloop).
Hearing Aid Definitions
Hearing Aid Terms Defined
Hearing Aid Style:
The type of hearing aid defined by its size and position relative to the ear. Common styles include behind-the-ear, receiver in-the-ear, and in-the-canal.
Hearing Loss Association of America (HLAA):
Informative resource on hearing loss and related topics.
High-frequency Hearing Loss:
The most common type of hearing loss. People with high-frequency hearing loss have the most difficulty hearing higher frequency sounds, like the sounds of speech.
In-the-canal (ITC) Hearing Aids:
Hearing aid with parts enclosed in a case that fits inside of the ear canal. Completely-in-the-canal (CIC) hearing aids are also available that are near invisible when worn.
In-the-ear (ITE) Hearing Aids:
Hearing aid with parts enclosed in a case that fits in the outer part of the ear.
Loop System:
A listening system consisting of a loop of wire placed around the perimeter of a designated area (room) and connected to an existing PA system for that space to transmit sound directly to hearing aids that have a telecoil program setting. It can also transmit to handheld receiver devices with headphones for individuals who do not have a telecoil equipped hearing aid. Used in churches, some libraries, and theaters.
Microphone:
The hearing aid component that picks up sound in the environment and converts the sound waves into an electrical signal.
Mixed Hearing Loss:
Hearing loss that is a combination of conductive and sensorineural losses.
Noise Reduction:
Functionality that assists the hearing aid to differentiate speech sounds from background noise, which results in the augmentation of speech and the inhibition of distracting noise.
Over-the-Counter (OTC) Hearing Aids:
Hearing aids that are available without a prescription. Intended for people with mild to moderate hearing losses only.
Receiver In-the-Ear and In-the-Canal (RIE/RIC) Hearing Aids:
Hearing aids which include a small component outside of the ear to capture incoming sounds which connects to a small speaker placed inside the ear canal.
Sensorineural Hearing Loss:
A type of hearing loss that occurs when there is damage to the nerve cells of the inner ear. This is the most common type of permanent hearing loss, triggered by being exposed to loud noise, the aging process, genetics, or other health issues. A person may “hear” sounds but had difficulty or is not able to understand speech.
Speaker:
The hearing aid component that delivers the enhanced sound to the ear.
Telecoils:
A coil placed inside of a hearing aid that allows it to connect to wireless signals originating from telephones, assistive listening devices, and hearing loops installed in public venues.
Threshold of Hearing:
The lowest decibel level that can be detected at each frequency.
Tinnitus:
A prolonged ringing or buzzing in the ears when no external sound is present. Usually a sign of hearing damage or loss.
Wireless Antenna:
Available in specific hearing aids, enabling wireless connectivity to compatible gadgets such as smartphones and music players.
Unilateral Hearing Loss:
Hearing loss which is only in one ear.
Variable Programming:
Hearing aid programming that enables the individual to adjust sound settings depending on the environment (e.g. at home versus in a chaotic restaurant).
DWD Contact Information
201 E. Washington Ave
P.O. Box 7946
Madison, WI 53707
(608) 266-3131
Sign up for DWD news and updates
A proud partner of the ![]() network
network